 A History lecturer teaching a class about the history of the Xhosa people in South Africa’s Eastern Cape province stops speaking English for a few minutes. She switches to isiXhosa, the home language of nearly 80% of the Eastern Cape’s residents…..more
A History lecturer teaching a class about the history of the Xhosa people in South Africa’s Eastern Cape province stops speaking English for a few minutes. She switches to isiXhosa, the home language of nearly 80% of the Eastern Cape’s residents…..more
Category Archives: News
News
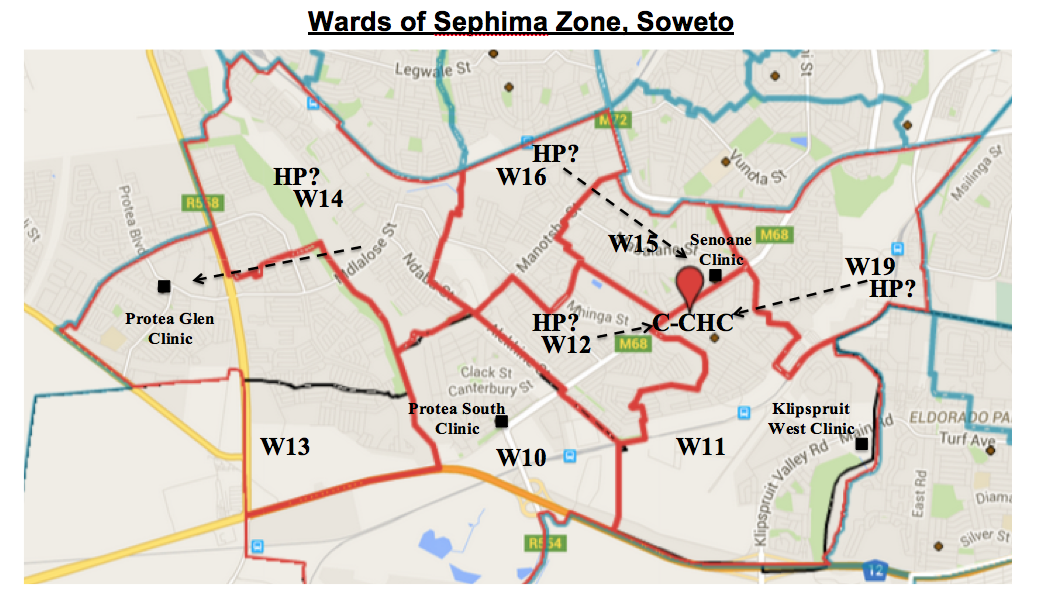
Chiawelo Community Practice to be rolled out in other wards in Chiawelo

Members of the Chiawelo Community Practice take a group picture with the MEC for Health in Gauteng, Qedani Mahlangu. The MEC had requested a presentation by Dr Shabir Moosa on Chiawelo Community Practice (CCP) to the senior managers of Gauteng Department of Health on Wednesday 20th May 2015. She insisted that the model be rolled out to all township wards in Gauteng by March 2016. The resources required are expected to be minimal but the change management may require more effort. The MEC requested Dr Moosa to champion the WBOT in Johannesburg and join a team of champions in other Districts, Dr Victor Figeuroa and Prof Jannie Hugo, to ensure the rollout. The immediate plan was to expand CCP from just ward 11 to other wards around the CHC: Wards 10,12,13,14,15,16 & 19, setting more such community practices in the CHC and clinics around.
WONCA president’s message on World Family Doctor Day 2015
New community health education films in Bemba
We are delighted to announce the release of 8 new community health education films in Bemba, for use by community health workers in Zambia in their work to build awareness of maternal and child health topics such as prevention of malaria, identifying warning signs in pregnancy, and basic newborn care.
Building on our project in the Chitambo District of central Zambia, where films have been screened at 14 rural health posts in addition to screenings at Chitambo Hospital, we have formalised a partnership with the Ministry of Community Development Mother Child Health to introduce the films into the neighbouring district of Serenje. The Ministry selected 8 films which they felt to be most useful in their outreach work, and these were previewed at seven different health facilities in Serenje at the end of April (Kabundi, Chibobo, Nchimishi, Mulilima, Kabamba, Kanona and Miswema.) Community screenings will follow at 66 rural health posts across Serenje, where outreach work takes place each month.
The films that are available are:
– Breastfeeding
– What and when to feed your child (6 – 24 months)
– What pregnant women need to eat
– Focused antenatal care
– Warning signs in pregnancy
– How to care for a newborn – the first hours after delivery
– Is your child sick – identifying signs of sickness and malaria, pneumonia and diarrhoea
– Cervical cancer – understanding prevention, screening and treatment
These films are free to view and use: http://medicalaidfilms.org/our-films/films-in-bemba/ and we hope that they will be of use to organisations working in Zambia.
Many thanks to the Ministry of Community Development Mother Child Health, Charles Hayward Foundation, and those who assisted with the translation and dubbing of the films.
For more information please contact Josie – Josie@medicalaidfilms.org
Josie Gallo
Content Co-ordinator
Medical Aid Films
Office: +44 (0) 20 7396 5327
Mobile: +44 (0) 7790 047694
16 Lincoln’s Inn Fields, London, WC2A 3ED, UK
David Werner: On training local people…
I have read with great interest your interchange over recommendations for lowering preventable maternal mortality. While Jon’s address from years back, outlining a multi-leveled approach ranging from home-based care by TBA through heath posts and rural clinics to hospitals, makes a lot of sense, it has nevertheless been hard to put into practice. Cultural and economic barriers (often including illicit under-the-table charges by professionals) often make the referrals to “higher” levels of care prohibitive for the families involved.
I therefore agree very much with Nick that training local people — including selected healthworkers and TBAs — to do some of the life-saving procedures usually reserved “for doctors only” would have potentially for significantly lowering child mortality.
Not everything need be or can be done at once. But some simple measures could make a substantial difference. For example “severe” postpartum bleeding is a major cause of maternal mortality in poor communities where up to 70% of women are visibly anemic, many of them severely so. Provision of oxytocics to TBAs, with adequate precautionary training to use only after the baby is delivered, could probably save a large number of women’s lives. (The training of lay providers needs to be better than that of doctors on this issue, where the premature overuse — often to speed up normal delivery — is a common malpractice leading to everything from vaginal tears to ruptured uteri to asphyxiation of the baby. Nevertheless, adequate instruction of TBAs on the proper use and warnings with oxytocics shouldn’t take more than half an hour.)
The major obstacle to systematically enabling lay practitioners to perform tasks exclusively reserved for titled “professionals” is the resistance from the medical establishment. Years ago I argued with the MOH directors in Colombia about the question of teaching health workers and TBAs to use oxytocin to control postpartum hemorrhage, and they were afraid to even consider it. This was not because they didn’t believe it could save many women’s lives, but because they feared the criticism they would get from the medical establishment if a mother died after a TBA used oxytocin — as was occasional likely to happen even though far more women’s lives would be saved. In short, the decision-makers in the MOH were more concerned about protecting themselves than about protecting the lives of poor rural women.
Nick is absolutely right that — given the many barriers to taking poor rural women to where they can get the professional care they need — a great many women’s lives could be saved by training local lay service providers to “specialize” in such life-saving techniques as C-sections and transfusions, use of blood thickeners, and the like. As Nick points out, there are many examples of village health workers and birth attendants learning and successfully practicing equally demanding skills. (For example see our Newsletter #76 on how a village boy in Mexico learned eye-surgery from a visiting ophthalmologist, and eventually became a eye-surgeon and professor of ophthalmology: http://web.healthwrights.org/newsletters/nl75-village-boy-to-eye-surgeon/)
In this context, the WHO has been a two edged sword. At least in some countries, it has counseled health ministries not to work with TBAs. When I visited East Timor in 2011 I found this to be the case. In our Newsletter # 69 I wrote:
“The Health Ministry’s failure to officially recognize Traditional Birth Attendants (TBAs) is another big obstacle to mother and child health in Timor-Leste. A graph published by the Health Ministry shows that about 20% of babies are delivered by health professionals in hospitals; nearly 30% are delivered by trained midwives (educated women officially trained in childbirth); and half of all babies are delivered by “other.” “Other” refers mostly to Traditional Birth Attendants, who do deliveries in homes and whom most mothers (including city dwellers) prefer. However, the graph doesn’t refer to them as TBAs because, following a directive of the World Health Organization, they are no longer recognized by the Timorese Health Ministry. Given that TBAs attend the vast majority of births in remote areas where the titled midwives almost never go, the WHO directive makes little sense. If the Ministry of Health provided basic support, back-up, and sterile birth kits to the TBAs, it could have a significant impact on maternal and child health. And the impact could be even greater if TBAs were encouraged to cooperate with Family Health Promoters in pre- and post natal care, including nutrition and immunization.” (http://healthwrights.org/index.php?option=com_content&view=article&layout=edit&id=228)
A Timorese obstetrician worked with upgrading the skills of TBAs in a remote area of the island, resulting in an impressive decline in maternal and neonatal mortality. The Japanese govt. development agency offered the Timorese MOH a million dollar grant to expand the program throughout remote highland areas. However the WHO disapproved, and the project never resulted.
Breaking the monopoly of medical establishment is still a major challenge in achieving adequate health care for the disadvantaged.
— David Werner
Mobile phones, childbirth and newborn care: The Safe Delivery App
The Safe Delivery App
http://maternity.dk/en/content/mhealth
‘As part of their focus on strengthening the quality of care through clinical trainings, “Maternity” has in partnership with University of Copenhagen and University of Southern Denmark developed an innovative smart-phone app called The Safe Delivery App. The Safe Delivery App is a mHealth Tool that teaches and instructs birth attendants in hard-to-reach areas how to manage normal and complicated deliveries through simple, animated clinical instruction films.’
—
Best wishes, Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
19th WHO Model List of Essential Medicines (April 2015)
The 19th WHO Model List of Essential Medicines is freely available here:
http://www.who.int/medicines/publications/essentialmedicines/EML2015_8-May-15.pdf
‘Increasingly, governments and institutions around the world are using the WHO list to guide the development of their own essential medicines lists, because they know that every medicine listed has been vetted for efficacy, safety and quality, and that there has been a comparative cost-effectiveness evaluation with other alternatives in the same class of medicines…’
http://www.who.int/medicines/news/eml_2015/en/
Best wishes,
Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
PLoS ONE: Mobile app to support antenatal care by CHWs in Nigeria
‘A low-cost mobile case management and decision support application can spur behavior change and improve the quality of services provided by a lower level cadre of healthcare workers.’ This is the conclusion of a paper in the open access journal PLoS ONE.
CITATION: Assessment of the Quality of Antenatal Care Services Provided by Health Workers Using a Mobile Phone Decision Support Application in Northern Nigeria: A Pre/Post-Intervention Study
Marion McNabb , Emeka Chukwu, Oluwayemisi Ojo, Navendu Shekhar, Christopher J. Gill, Habeeb Salami, Farouk Jega
Published: May 5, 2015DOI: 10.1371/journal.pone.0123940
ABSTRACT
Background: Given the shortage of skilled healthcare providers in Nigeria, frontline community health extension workers (CHEWs) are commonly tasked with providing maternal and child health services at primary health centers. In 2012, we introduced a mobile case management and decision support application in twenty primary health centers in northern Nigeria, and conducted a pre-test/post-test study to assess whether the introduction of the app had an effect on the quality of antenatal care services provided by this lower-level cadre.
Methods: Using the CommCare mobile platform, the app dynamically guides CHEWs through antenatal care protocols and collects client data in real time. Thirteen health education audio clips are also embedded in the app for improving and standardizing client counseling. To detect changes in quality, we developed an evidence-based quality score consisting of 25 indicators, and conducted a total of 266 client exit interviews. We analyzed baseline and endline data to assess changes in the overall quality score as well as changes in the provision of key elements of antenatal care.
Results: Overall, the quality score increased from 13.3 at baseline to 17.2 at endline (p<0.0001), out of a total possible score of 25, with the most significant improvements related to health counseling, technical services provided, and quality of health education.
Conclusion: These study results suggest that the introduction of a low-cost mobile case management and decision support application can spur behavior change and improve the quality of services provided by a lower level cadre of healthcare workers. Future research should employ a more rigorous experimental design to explore potential longer-term effects on client health outcomes.
—
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Why Facebook’s News Experiment Matters to Readers
 Facebook’s new plan to host news publications’ stories directly is not only about page views, advertising revenue or the number of seconds it takes for an article to load. It is about who owns the relationship with readers…..more
Facebook’s new plan to host news publications’ stories directly is not only about page views, advertising revenue or the number of seconds it takes for an article to load. It is about who owns the relationship with readers…..more
PLoS ONE: Men’s Knowledge of Obstetric Danger Signs, Birth Preparedness and Complication Readiness in Rural Tanzania.
‘There is a need to have innovative strategies that increase awareness of danger signs as well as birth preparedness and complication readiness among men.’
Please see below the citation and abstract of a new paper in the open access journal PLoS ONE.
CITATION: August F, Pembe AB, Mpembeni R, Axemo P, Darj E (2015) Men’s Knowledge of Obstetric Danger Signs, Birth Preparedness and Complication Readiness in Rural Tanzania. PLoS ONE 10(5): e0125978. doi:10.1371/journal.pone.0125978
ABSTRACT
Background: Men’s involvement in reproductive health is recommended. Their involvement in antenatal care service is identified as important in maternal health. Awareness of obstetric danger signs facilitates men in making a joint decision with their partners regarding accessing antenatal and delivery care. This study aims to assess the level of knowledge of obstetric complications among men in a rural community in Tanzania, and to determine their involvement in birth preparedness and complication readiness.
Methods: A cross-sectional survey was conducted where 756 recent fathers were invited through a two-stage cluster sampling procedure. A structured questionnaire was used to collect socio-demographic characteristics, knowledge of danger signs and steps taken on birth preparedness and complication readiness. Data were analyzed using bivariate and multivariable logistic regression to determine factors associated with being prepared, with statistically significant level at p<0.05.
Results: Among the invited men, 95.9% agreed to participate in the community survey. Fifty-three percent could mention at least one danger sign during pregnancy, 43.9% during delivery and 34.6% during the postpartum period. Regarding birth preparedness and complication readiness, 54.3% had bought birth kit, 47.2% saved money, 10.2% identified transport, 0.8% identified skilled attendant. In general, only 12% of men were prepared. Birth preparedness was associated with knowledge of danger signs during pregnancy (AOR = 1.4, 95% CI: 1.8-2.6). It was less likely for men living in the rural area to be prepared (AOR=0.6, 95% CI; 0.5-0.8).
Conclusion: There was a low level of knowledge of obstetric danger signs among men in a rural district in Tanzania. A very small proportion of men had prepared for childbirth and complication readiness. There was no effect of knowledge of danger signs during childbirth and postpartum period on being prepared. Innovative strategies that increase awareness of danger signs as well as birth preparedness and complication readiness among men are required. Strengthening counseling during antenatal care services that involve men together with partners is recommended.
—
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Quality of care for pregnant women and newborns — the WHO vision
‘To end preventable maternal and newborn morbidity and mortality, every pregnant woman and newborn need skilled care at birth with evidence-based practices delivered in a humane, supportive environment.’
Please find below extracts of a Commentary in the BJOG International Journal of Obstetrics and Gynaecology. The full text is freely available here:
http://onlinelibrary.wiley.com/doi/10.1111/1471-0528.13451/epdf
(Thanks to WHO’s new open access policy http://www.who.int/about/policy/en/ all external articles by WHO staff are published open access)
CITATION: Quality of care for pregnant women and newborns — the WHO vision
Tunçalp, WM Were, C MacLennan, OT Oladapo, AM Gülmezoglu, R Bahl, B Daelmans, M Mathai, L Say, F Kristensen, M Temmerman and F Bustreo
Article first published online: 1 MAY 2015
DOI: 10.1111/1471-0528.13451
‘Moving beyond 2015, the World Health Organization (WHO) envisions a world where ‘every pregnant woman and newborn receives quality care throughout pregnancy, childbirth and the postnatal period.’…’‘Based on the current evidence on burden and impact, the following specific thematic areas have been identified as high priority for this vision:
- Essential childbirth care including labour monitoring and action and essential newborn care at birth and during the first week
- Management of pre-eclampsia, eclampsia and its complications;
- Management of postpartum haemorrhage;
- Management of difficult labour by enabling safe and appropriate use of medical technologies during childbirth;
- Newborn resuscitation;
- Management of preterm labour, birth and appropriate care for preterm and small babies;
- Management of maternal and newborn infections.’
‘In this vision, WHO will use a QoC improvement strategy, an adaptation of the ‘Plan-Do-Study Act’ (PDSA) cycle model based on evidence synthesis, best practice and experience.’
—
Best wishes,
Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Health Ethics Initiative: Health advocacy, right to health, quality of healthcare
A couple of us at Johns Hopkins and beyond are creating an online platform that uses storytelling as a medium of social reform and dialog in health ethics in low and middle-income countries.
We believe that amidst growing inequality in access to medical treatment, malpractice, lack of accountability, loss of human dignity and capricious health policy and practice, a global discourse on the values driving healthcare in the “global south” has become necessary.
Our online forum, which is to launch soon, examines ethical failures, achievements and everything in between. The stories we hope to publish simultaneously probe, heal and offer food for thought without being punitive or judgmental.
Have a story? We are looking for ingenious writers based in a developing country (or with strong ties to one) who can produce first-person (non-fiction) vignettes (150 words or less) that illustrate: an ethical dilemma faced by a person in a health profession (broadly defined) in a developing country, the context, how the person acted and why, and what the aftermath was.
Potential stories of interest could cover a wide range of health issues (health advocacy, right to health, quality of healthcare, knowledge of healthcare) and come from individuals in hospitals, medical campuses, businesses all along the pharmaceutical supply chain, public health workers, members of NGOs or other public/private health groups, lawyers and lawmakers, and beyond. We also accept narratives and qualitative material that derive from your research and other professional and personal experiences.
While some stories will be squarely entrenched in the “right” or “wrong” ethical camp, we expect the best narratives to straddle the fine line in between. A representative picture or two to accompany your short story would be ideal.
This is an all-volunteer project for the moment (we aren’t paying ourselves either); however, we plan to compensate our regular contributors retroactively upon receiving funding.
Should you be interested, feel free to contact me at pagrawa6@jhu.edu or at valueofabeing@gmail.com. Send us a brief bio and how you think you can contribute.
Regards,
Priyanka.
HIFA profile: Priyanka Agrawal is a doctor at the Johns Hopkins Bloomberg School of Public Health in the USA. Email address: valueofabeing AT gmail.com
Guinea Ebola diary: In the land of lost handshakes

Nigeria people’s manifesto: Health
The health statistics in Nigeria make chilling reading. Malaria scythes its way through the population, hitting the most vulnerable hardest. UNICEF says it kills 250,000 children under the age of five each year, a scandal in a country where foreign-exchange reserves topped $60bn in 2008. Mortality levels are among the highest in the world, with life expectancy at 48 years. Preventable diseases find easy victims in Nigeria – and rapid urbanisation is creating fresh problems……more
Pneumococcal vaccine cuts hospitalisations by 70 percent
 New data shows that South Africa’s expensive pneumococcal vaccine roll out has cut childhood hospitalisations due to meningitis, pneumonia and rotavirus by about 70 percent in just five years, according to Minister of Health Dr Aaron Motsoaledi…..more
New data shows that South Africa’s expensive pneumococcal vaccine roll out has cut childhood hospitalisations due to meningitis, pneumonia and rotavirus by about 70 percent in just five years, according to Minister of Health Dr Aaron Motsoaledi…..more
More than 3,000 await cataract surgeries
 The Gauteng Department of Health has almost halved the number of people awaiting sight-restoring cataract operations in the last year but more than 3,000 people are still waiting for their turn to see again….more
The Gauteng Department of Health has almost halved the number of people awaiting sight-restoring cataract operations in the last year but more than 3,000 people are still waiting for their turn to see again….more
SA’s emerging entrepreneurs ‘among the best in the world’
RENOWNED international businessman Rich Benton has lauded SA’s emerging entrepreneurs as being among “the best in the world”. Mr Benton — one of the founding directors of the UK’s Capita Group and chair of the Global Social Entrepreneur Network — advised SA to groom budding business brains in their formative years….more . See more about Lifeco
Residents of Soweto march on Eskom
MORE than 1,000 Soweto residents, most of them in African National Congress colours, gathered at the Hector Pieterson Museum on Thursday before officials of the ruling party led a march to Eskom’s offices in Diepkloof, where a memorandum was delivered. Jolidee Matongo, ANC chairman in Johannesburg, said the party did not oppose the prepaid system that the utility has sought to instal in Soweto, but that the parastatal had failed to consult Orlando West residents over it…..more
New resource available: Workers Guide to Health and Safety
On International Workers’ Day, the Berkeley, CA-based health publisher Hesperian released a one-of-a-kind resource on workers’ health and safety. More than a decade in the making and drawing on the experiences of workers and health educators from every continent, this book aims to provide essential information to workers themselves, those who are the best placed and the most highly motivated to prevent the devastating factory disasters that all too often dominate the news.
The Workers’ Guide to Health and Safety provides occupational safety and health information in an accessible, well-illustrated format that speaks directly to workers’ experience. While covering workplace problems such as electrical hazards, machine dangers, ergonomics, chemical use, fire, among others, it also breaks new ground by also focusing on “social hazards”: low wages, long hours, sexual harassment, workplace violence, and other problems that affect factory workers’ health but are usually not considered part of occupational health and safety.
The book also covers specific illnesses that are common or exacerbated by factory conditions, such as HIV, tuberculosis, and mental health.
For a complete description of the book, a table of contents, and sample chapters, go to:
http://hesperian.org/books-and-resources/workers-guide-to-health-and-safety/
Despite the fact that most people spend the majority of their waking hours involved in working, this is one of the first resources to take a global look at the health problems caused by work and place them into a primary care context. PHM has long expressed interest in including worker health in its organizing efforts. This book provides activists with information and a framework for doing so.
Guy Ryder, Director-General of the International Labour Organization, has recognized the book as “an excellent resource in helping workers achieve safe and dignified jobs. The Workers’ Guide to Health and Safety is full of innovative and sustainable ways for workers, employers, and consumers to make that right a reality.” This is important, he continued, because “Globally, an estimated 2.3 million workers die every year from injuries at work and work related diseases. Many millions more are harmed by their work. This represents a colossal social and economic burden for enterprises, communities and countries, not to mention an appalling human and financial problem for workers and their families.”
Like all of Hesperian’s materials, the book has been extensively field-tested in 25 countries to ensure it will be as useful as possible. The experience of training workers using early drafts of the book led Sanjiv Pandita, Director of the Asia Monitor Resource Centre in Hong Kong, to say: “This book has already empowered hundreds of workers involved in its field-testing across Asia. Hundreds of thousands of people throughout Asia need and will benefit from this book.”
Not a dry text about occupational safety, every chapter in the Workers’ Guide includes real stories about how workers have organized to improve conditions in the workplace and in the community, and the descriptions of the struggles of women and migrant workers make this book as timely as tomorrow’s headlines. The book also includes activities to involve workers in measuring and responding to hazards on the job. Finally, an extensive chemical index presents complex chemical information in a manner that is easy to understand that allows workers to identify chemicals they may be working with, understand their short-term and chronic health effects, and propose various ways to protect themselves by substituting safer chemicals, improving ventilation, and using the right personal protective equipment.
The 3 co-authors — Todd Jailer and Miriam Lara-Meloy (both members of PHM-USA), and Maggie Robbins — are all based in the San Francisco Bay Area, have a wealth of experience in working on issues of health, safety, and workplace organizing.
—
Todd Jailer, Managing Editor
Hesperian Health Guides
Knowledge for action.
Action for health.
CHWs support Patients Post Surgery in Haiti
CHW Central [http://www.chwcentral.org/] has posted a new feature: Can CHWs address access and outcome measurement challenges in surgical care? Experience from Haiti. [http://www.chwcentral.org/blog/can-chws-address-access-and-outcome-measurement-challenges-surgical-care-experience-haiti] The Lancet Commission on Global Surgery* reveals that five billion people, as many as nine of ten individuals in low and middle-income countries, lack access to safe, affordable surgical care. This affects the poor, marginalized, and rural populations who have limited funds, long distances to care and poor travel infrastructure. If they do reach care, there are often no surgeons or anesthetists, medications, oxygen, or blood.
Dr. Alexi Matousek states that global surgery faces two main crises: lack of access to surgical services for vulnerable populations and an inability to measure outcomes that would enable quality improvement. He believes CHWs can be used to address both these issues. He developed a program to use CHWs as surgical accompagnateurs who could link patients to care. Accompagnateurs received mountain patients at the hospital, and took them through every step and location in the hospital to be evaluated for surgery, including financial support. This simple intervention increased the elective operation rate four- fold for this vulnerable population.
Dr. Maotusek also developed a Community Outcomes Measurement program using a mobile application that enables CHWs to administer a questionnaire on symptoms of infection, obtain GPS data and submit a high-quality photograph of the incision three times during the 30 days after an operation.
The long-term goal is to assess whether CHWs with mobile phones could replace the need for surgeons to perform outpatient follow up for patients who have no symptoms of infection, and also to evaluate whether mobile health follow up can identify infections earlier than the current standard of care, leading to reduced morbidity.
See the full article and video at CHW Central. [http://www.chwcentral.org/]
*Meara, JG, Leather, AJM, Hagander, L et al. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015; (published online April 27.)
Donna Bjerregaard
Senior Technical Advisor
Initiatives Inc.
264 Beacon Street
Boston, MA 02116
Tel: 617 262 0293
Fax: 617 262 2514
