 E-maintenance leaves clinic in shambles. When the Gauteng portfolio committee visited a state clinic on the West Rand, it found broken equipment galore. The boom and motor gate at the entrance to the clinic remains broken, even though the damage was reported via the e-maintenance system in November last year. Though the clinic was squeaky clean, the glass panels of a door in the main passageway were broken. This, too, had been reported in November…..more
E-maintenance leaves clinic in shambles. When the Gauteng portfolio committee visited a state clinic on the West Rand, it found broken equipment galore. The boom and motor gate at the entrance to the clinic remains broken, even though the damage was reported via the e-maintenance system in November last year. Though the clinic was squeaky clean, the glass panels of a door in the main passageway were broken. This, too, had been reported in November…..more
Author Archives: Shabir Moosa
Training Resources Bulletin, September 2015
The new Training Resources Bulletin from AIHA is available now at : http://www.hifa2015.org/wp-content/uploads/TrainingResourcesBulletinSept15.pdf
Training Resources Bulletin
September 2015
American International Health Alliance
Knowledge Management Program
The Training Resources Bulletin is intended to assist institutions and individuals who are seeking online training options in the field of medicine, public health, social work, and related topics. If this document is to be redistributed or posted on another Web site, we request that it be posted in full/without alteration, and that credit is given to the American International Health Alliance as the source of the document.
Your input (including new sources of online training opportunities) will be greatly appreciated.
Previous issues are available at http://www.healthconnect-intl.org/resources.html
In This Issue …
ONLINE COURSES
– Health Literacy and Communication for Health Professionals
– Basic course on Evidence Based Medicine (EBM)
– Ethical Challenges in Short-Term Global Health Training
– Finding, organizing and using health information
TRAINING MATERIALS
– Implementation research toolkit
– Introduction to Nursing Part 2
– ORB
– ENGAGE-TB
Irina Ibraghimova, PhD
Library and Information Management Specialist,
HealthConnect International
Costs and cost-effectiveness of community health workers: evidence from a literature review
Diana Frymus said: ‘Better data on CHWs would help demonstrate their impact and cost-effectiveness’. This is corroborated by one of the new papers in the open-access journal Human Resources for Health. Below is the citation and abstract. The paper points to a relative lack of evidence / data on the cost-effectiveness of CHWs in the situations where they are most deployed, with the exception of tuberculosis.
Diana again: ‘There are still many policy makers who are skeptical of the value of CHWs. If we can demonstrate their value, we can get CHWs added as a formal member of the health team, with proper support supervision, a career ladder, and a salary.’ Clearly, stronger evidence of their cost-effectiveness would greatly help to convince policymakers to invest more in CHW scale-up.
CITATION: Costs and cost-effectiveness of community health workers: evidence from a literature review
Kelsey Vaughan1*, Maryse C Kok1, Sophie Witter2 and Marjolein Dieleman1
* Corresponding author: Kelsey Vaughan kvaughan@gmail.com
Human Resources for Health 2015, 13:71 doi:10.1186/s12960-015-0070-y
The electronic version of this article is the complete one and can be found online at: http://www.human-resources-health.com/content/13/1/71
ABSTRACT
Objective: This study sought to synthesize and critically review evidence on costs and cost-effectiveness of community health worker (CHW) programmes in low- and middle-income countries (LMICs) to inform policy dialogue around their role in health systems.
Methods: From a larger systematic review on effectiveness and factors influencing performance of close-to-community providers, complemented by a supplementary search in PubMed, we did an exploratory review of a subset of papers (32 published primary studies and 4 reviews from the period January 2003–July 2015) about the costs and cost-effectiveness of CHWs. Studies were assessed using a data extraction matrix including methodological approach and findings.
Results: Existing evidence suggests that, compared with standard care, using CHWs in health programmes can be a cost-effective intervention in LMICs, particularly for tuberculosis, but also – although evidence is weaker – in other areas such as reproductive, maternal, newborn and child health (RMNCH) and malaria.
Conclusion: Notwithstanding important caveats about the heterogeneity of the studies and their methodological limitations, findings reinforce the hypothesis that CHWs may represent, in some settings, a cost-effective approach for the delivery of essential health services. The less conclusive evidence about the cost-effectiveness of CHWs in other areas may reflect that these areas have been evaluated less (and less rigorously) than others, rather than an actual difference in cost-effectiveness in the various service delivery areas or interventions. Methodologically, areas for further development include how to properly assess costs from a societal perspective rather than just through the lens of the cost to government and accounting for non-tangible costs and non-health benefits commonly associated with CHWs.
—
Best wishes, Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
All fired up about the wiring of the human brain
STEPH Vermeulen, pioneer in EQ — emotional intelligence — has spent the century so far studying research on brains. Now, in one short book, she’s turning the approach to grey matter upside down. We no longer talk about EQ versus IQ, says Vermeulen, whose book on emotional intelligence, published 15 years ago was a bestseller. “But, we realise now we need both our intelligent and emotional quotients to innovate, to create new technology and carve out new worlds and lives.” Hence her latest book, Personal Intelligence: Future Fit Now, which she describes as “EQ all grown up”….more
Gauteng Health has not won a single lawsuit
 With not a single lawsuit decided in their favour, the Gauteng Health Department is haemorrhaging money – and it seems this isn’t about to stop. Health MEC Qedani Mahlangu revealed this week in the Gauteng Legislature that her department had forked out R544 million to date for medical negligence claims. These claims date back to 2010. According to information from the MEC, 168 cases had been lost in court while eight had been settled out of court. The individual cases make for harrowing reading. DA shadow MEC for Health in Gauteng Jack Bloom, who posed the questions to Mahlangu, carries a dossier on these claims. Many of them point to negligence of a shocking nature…..more
With not a single lawsuit decided in their favour, the Gauteng Health Department is haemorrhaging money – and it seems this isn’t about to stop. Health MEC Qedani Mahlangu revealed this week in the Gauteng Legislature that her department had forked out R544 million to date for medical negligence claims. These claims date back to 2010. According to information from the MEC, 168 cases had been lost in court while eight had been settled out of court. The individual cases make for harrowing reading. DA shadow MEC for Health in Gauteng Jack Bloom, who posed the questions to Mahlangu, carries a dossier on these claims. Many of them point to negligence of a shocking nature…..more
Definitions and training of CHWs
CTCs are defined as ‘health workers who carry out promotional, preventive and/or curative health services and who are often the first point of contact at community level in countries in the global south… usually have at least a minimum level of training in the context of the intervention that they carry out and include a broad variety of health workers, including community health workers (CHWs) and auxiliary health workers.’
For the benefit of those who may not have immediate web access, below is the preamble. There are several interesting-looking case studies, reviews and research articles. If anyone can provide comments on the collection as a whole, or on individual papers, please send a message to hifa2015@dgroups.org
‘CTC providers are strategically placed as the interface between health systems and the communities they serve. National and international decision-makers are once again turning to (CTC) services in order to strengthen health systems in the context of the momentum generated by strategies to support universal access, delivery of the Millennium Development Goals (MDGs) and the post-MDG agenda. However there are a number of flaws in current systems that need to be better understood. We are at a critical stage in the development of CTC programming and policy which requires the creation and communication of new knowledge to ensure the safety, sustainability, quality and accessibility of services, and their links with both the broader health system and the communities that CTC’s serve.
‘The series covers a range of topics on close to community providers for health systems development, including, but not limited to, the following:
‘Conceptualising the range of CTC providers in different contexts
Methods and tools for analysing CTC programmes
Cost effectiveness of CTC programmes
Challenges and opportunities CTC providers face in reaching and supporting marginalised groups
Diverse community perspectives and ownership of CTC programmes
Opportunities for CTC providers to act as champions for social change
The interface between health systems and CTC programmes
Strategies to motivate, retain and sustain CTC providers
Integrating vertical programmes using CTC providers within national programmes’
—
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Chiawelo Community Practice reports at Ward Councillor community meeting
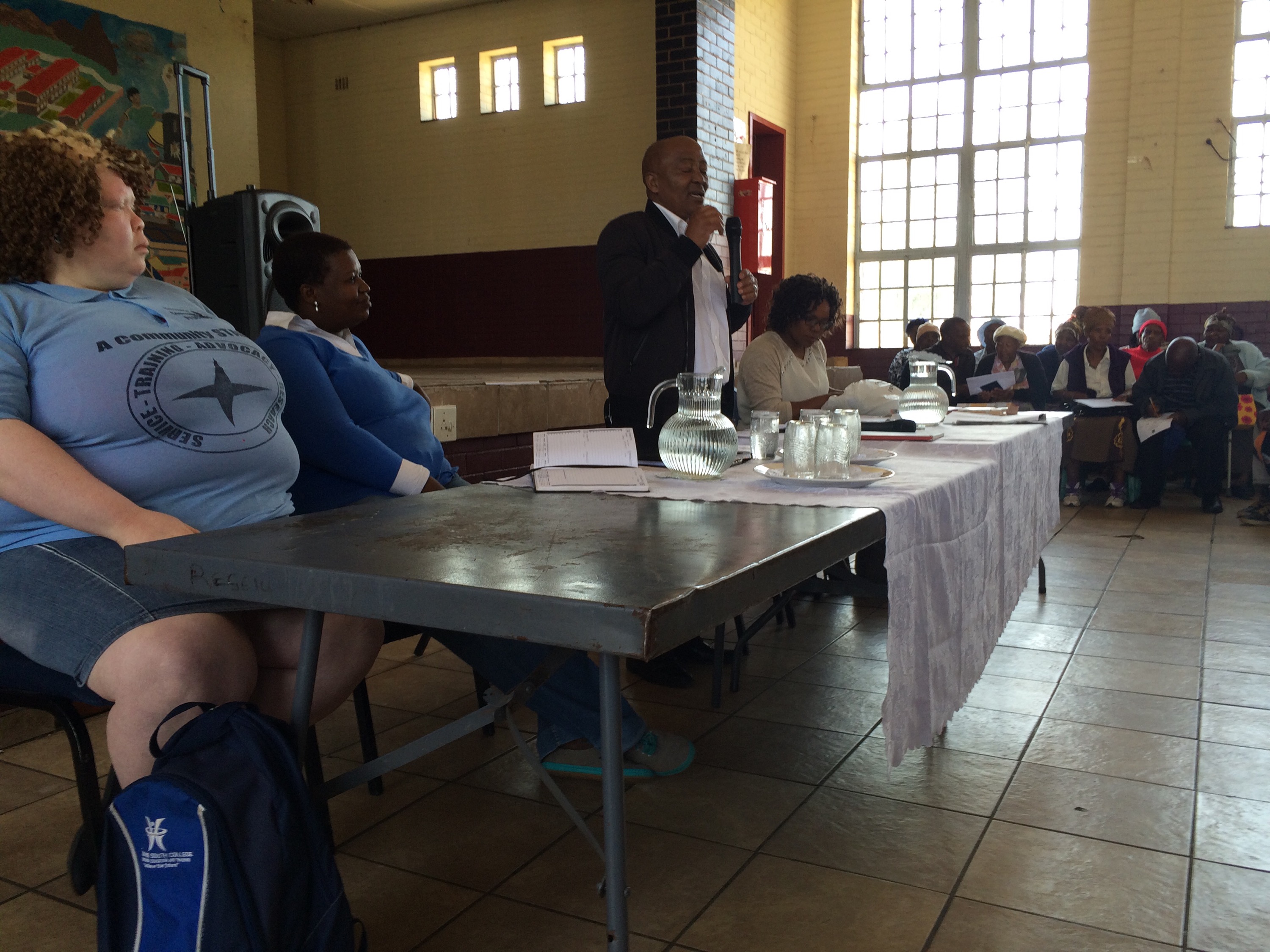
 Dr. Moosa addresses 350+ residents in Ward 15, Soweto called by Cllr Dube to discuss challenges with social grants and the changes with PHC Re- engineering & COPC plans as premised on Chiawelo Community Practice. COPC welcomed but lots of issues with children abuse of grants and unwelcome deductions with BEE service provider.
Dr. Moosa addresses 350+ residents in Ward 15, Soweto called by Cllr Dube to discuss challenges with social grants and the changes with PHC Re- engineering & COPC plans as premised on Chiawelo Community Practice. COPC welcomed but lots of issues with children abuse of grants and unwelcome deductions with BEE service provider.
CHW Data for Decision Making – Challenges for scale-up of CHW programs
I have been following with interest the first few days of the debate on “CHW data for decision making”. Some of the contributions go to the heart of the matter, which is that at present unfortunately community health workers and other types of community-based practitioners sit at the margin of health systems: not formally recognized, not adequately trained, not properly incentivized, supervised or managed, not adequately counted or monitored.
There are clearly some missed opportunities in this, as the potential of these cadres in some settings to contribute to expand access to some essential health services and improve health outcomes is by now well recognized. Recent research, coordinated by the Global Health Workforce Alliance, has focused on assessing the cost-effectiveness of health programmes led by various types of community-based practitioners, finding that these cadres can represent a cost-effective policy options in some contexts (Mc Pake et al, WHO Bull 2015 http://www.who.int/bulletin/volumes/93/9/14-144899.pdf?ua=1). The case for investment in these cadres in some contexts has therefore a stronger empirical basis now.
However, support for community based practitioners should not take the form of one-off vertical initiatives disjointed from the rest of the health system: national governments that consider community-based practitioners a relevant policy option for their country contexts should invest – and be supported by the international community – in order to ensure that these cadres are adequately supported by and integrated in the health system. As Campbell et al note in a recent editorial (http://www.who.int/bulletin/volumes/93/9/15-162198.pdf?ua=1), maximizing the impact of community-based practitioners entails that (i) national policy-makers move towards the full integration of community-based practitioners in public health strategies, allowing these cadres to benefit from formal employment, education, health system support, regulation, supervision, remuneration and career advancement opportunities; (ii) development partners and funding agencies see the value of investing in these cadres and contribute to the capital and recurrent costs incurred when expanding this workforce; (iii) normative agencies such as WHO and ILO address the evidence and classification gaps by developing more precise definitions and categories for these cadres.
Related to this last point, which some of you already commented on, WHO is planning on developing guidelines on the role, education and integration of community-based practitioners for publication in 2017.
Many of the participants in this conversation have also commented on the need to ensure that we have better data on community health workers and other types of community-based practitioners. Efforts at developing better metrics for these important cadres should take place in the context of broader initiatives to enhance health workforce information systems.
WHO’s emerging Global Strategy on Human Resources for Health: Workforce 2030 (http://www.who.int/hrh/resources/online_consult-globstrat_hrh/en/), to be considered by the World Health Assembly in May 2016, calls for investments in strengthening country analytical capacities of HRH and health system data on the basis of policies and guidelines for standardization and interoperability of HRH data. The GSHRH puts forward the adoption of a National Health Workforce Account (NHWA) as a harmonized, integrated approach for annual and timely collection of health workforce information (http://www.who.int/hrh/documents/brief_nhwfa/en/). This approach, or related ones to strengthen health workforce metrics, should be extended to cover also community-based practitioners.
Best wishes,
Giorgio
HIFA profile: Giorgio Cometto is a Technical Officer at the World Health Organization in Switzerland. Professional interests: Human resources for health. comettog AT who.int
Reproductive Health Matters: Special Issue on knowledge, evidence, practice and power
Reproductive Health Matters: Special Issue on knowledge, evidence, practice and power
Editors: Shirin Heidari & Marge Berer
Reproductive Health Matters, Vol. 23, Issue 45, May 2015
http://www.rhm-elsevier.com/issue/S0968-8080%2815%29X0003-6
‘In this issue, “Reproductive Health Matters” is proud to publish a diverse range of findings from research projects and perspectives that highlight the complexities, strengths and weaknesses of the process of knowledgecreation and uncover the frequent disconnect between research, policies and practices, elaborating on its implications. The theme of this issue extends beyond knowledge production and engages with the domain of evidence-based policy and practice. As Johann Wolfgang von Goethe has said, “Knowing is not enough, we must apply; willing is not enough, we must act.”‘
—
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Int J Public Health: What research tells us about knowledge transfer strategies to improve public health in low-income countries
CITATION: What research tells us about knowledge transfer strategies to improve public health in low-income countries: a scoping review
by Stéphanie Siron, Christian Dagenais, Valéry Ridde
International Journal of Public Health -First online: 23 August 2015
http://link.springer.com/content/pdf/10.1007%2Fs00038-015-0716-5.pdf
Contact: S. Siron. e-mail: stephanie.siron@umontreal.ca
‘This study describes the current state of research on knowledge transfer strategies to improve public health in low-income countries, to identify the knowledge gaps on this topic. The review provides specific elements for understanding the transfer processes in low-income countries and highlights the need for systematic evaluation of the conditions for research results utilization.’
ABSTRACT
Objectives: This study describes the current state of research on knowledge transfer strategies to improve public health in low-income countries, to identify the knowledge gaps on this topic.
Methods: In this scoping review, a descriptive and systematic process was used to analyse, for each article retained, descriptions of research context and methods,
Results: 28 articles were analysed. They dealt with the evaluation of transfer strategies that employed multiple activities, mostly targeting health professionals and women with very young children. Most often these studies used quantitative designs and measurements of instrumental use with some methodological shortcomings. Results were positive and suggested recommendations for improving professional practices, knowledge and health-related behaviours. The review highlights the great diversity of transfer strategies used, strategies and many conditions for knowledge use.
Conclusions: The review provides specific elements for understanding the transfer processes in low-income countries and highlights the need for systematic evaluation of the conditions for research results utilization.
—
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Health Policy and Planning: Taking knowledge users’ knowledge needs into account in health
ABSTRACT
The increased demand for evidence-based practice in health policy in recent years has provoked a parallel increase in diverse evidence-based outputs designed to translate knowledge from researchers to policy makers and practitioners. Such knowledge translation ideally creates user-friendly outputs, tailored to meet information needs in a particular context for a particular audience. Yet matching users’ knowledge needs to the most suitable output can be challenging. We have developed an evidence synthesis framework to help knowledge users, brokers, commissioners and producers decide which type of output offers the best ‘fit’ between ‘need’ and ‘response’. We conducted a four-strand literature search for characteristics and methods of evidence synthesis outputs using databases of peer reviewed literature, specific journals, grey literature and references in relevant documents. Eight experts in synthesis designed to get research into policy and practice were also consulted to hone issues for consideration and ascertain key studies. In all, 24 documents were included in the literature review. From these we identified essential characteristics to consider when planning an output – Readability, Relevance, Rigour and Resources—which we then used to develop a process for matching users’ knowledge needs with an appropriate evidence synthesis output. We also identified 10 distinct evidence synthesis outputs, classifying them in the evidence synthesis framework under four domains: key features, utility, technical characteristics and resources, and in relation to six primary audience groups—professionals, practitioners, researchers, academics, advocates and policy makers. Users’ knowledge needs vary and meeting them successfully requires collaborative planning. The Framework should facilitate a more systematic assessment of the balance of essential characteristics required to select the best output for the purpose.
KEY MESSAGES
The increased demand for evidence-based health policy in recent years has provoked a parallel increase in diverse evidence-based outputs designed to translate knowledge from researchers to policy makers and practitioners, yet matching users’ specific knowledge needs to the most suitable output, while essential, can be challenging.
We have developed an evidence synthesis framework classifying 10 distinct evidence synthesis outputs under four domains: key features, utility, technical characteristics and resources, in relation to six primary groups of users: professionals, practitioners, researchers, academics, advocates and policy makers.
We propose a process for matching users’ knowledge needs with an appropriate evidence synthesis output, using essential characteristics to consider when planning an output: Readability, Relevance, Rigour and Resources. [Resources available for production (including time, funding and personnel]
When used in combination, the framework and process should facilitate a more systematic assessment of the balance of essential characteristics required to select the best output for the purpose and help knowledge users, brokers, commissioners and producers decide the best ‘fit’ between ‘need’ and ‘response’.
The full text is freely available here: http://heapol.oxfordjournals.org/content/early/2015/08/31/heapol.czv079.full?papetoc
CITATION: Taking knowledge users’ knowledge needs into account in health: an evidence synthesis framework
Deepthi Wickremasinghe, Shyama Kuruvilla, Nicholas Mays and Bilal Iqbal Avan,*
Health Policy Plan. (2015)
doi: 10.1093/heapol/czv079
Corresponding author. E-mail: bilal.avan@lshtm.ac.uk
New WHO publication: Brief Sexuality-related Communication
SUMMARY
‘Both research and consultations over the last decades have identified sexuality-related communication as an issue that requires urgent attention. While clients would like their health-care providers to discuss sexual health concerns, health workers lack the necessary training and knowledge to feel comfortable addressing such issues. This guideline provides health policy-makers and decision-makers in health professional training institutions with advice on the rationale for health-care providers’ use of counselling skills to address sexual health concerns in a primary health care setting.
The publication makes two main recommendations:
1. BSC [Behavioural and Social Change] is recommended for the prevention of sexually transmitted infections among adults and adolescents in primary health services
Quality of evidence: low – moderate
Strength of recommendation: strong
2. Training of health-care providers in sexual health knowledge and in the skills of brief sexuality-related communication is recommended.
Quality of evidence: low – very low
Strength of recommendation: strong
SELECTED EXTRACTS (selected by Neil PW)
‘The ability of people to achieve sexual health and well-being depends, among other things, on their access to comprehensive information about sexuality, their knowledge about the risks they face, and their vulnerability to the adverse consequences of sexual activity. To achieve sexual health, people also need opportunities for social support, access to good-quality sexual health care (i.e. addressing all elements of sexual health according to the WHO working definition, including products and materials), and an environment that affirms and promotes sexual health for all. These include counselling and communication programmes.’
‘Adolescents have the right to seek and receive information. In the absence of the information, support and skills needed to promote and protect their health and well-being, adolescents can suffer harms such as stigma, sadness, shame, guilt and anxiety, as well as STIs and unintended pregnancies.’
The full text is freely available here:
http://apps.who.int/iris/bitstream/10665/170251/1/9789241549004_eng.pdf?ua=1
—
Best wishes, Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
Announcing BMJ Global Health
I’m delighted to announce to HIFA members our new journal – BMJ Global Health – gh.bmj.com
The journal’s aims are to achieve a world in which every person and country has access to the information about health, health care and social determinants of health that they need to protect their own health and the health of the people for whom they take responsibility.
Everything that we do at BMJ is driven by our vision of “A Healthier World”. The journal will appeal to anyone working in global health – from doctors, nurses, healthcare workers, policy makers, researchers, NGOs and funders – as we work together to achieve this vision.
Please read the introductory Editorial from our Editor-in Chief Dr Seye Abimbola http://goo.gl/yP5ZTp
Access to the journal will be free to everyone – wherever they are in the world. In order to achieve this we need to work with funders which are willing to support our vision and to contribute to underwriting the costs of publishing a top quality journal. We welcome the opportunity to discuss how we can work together, so please spread the word.
The journal is accepting submissions now and the first content will go live in early 2016.
If you have any questions, want to submit an article or want to discuss supporting the journal, please contact me or Dr Seye Abimbola.
We hope that you agree that this is an important step forward in achieving a healthier world.
Sincerely
Peter Ashman
Publishing Director – BMJ
Patient education in the web page of MD Current India
Patient education is very important even in remote and rural areas. It is interesting that even those in remote and rural areas who do not know English are able to access information from internet through friends and relatives who know English.
There is a section for Patient education in the web page of MD Current India
http://mdcurrent.in/camps-and-rural-healthcare/
and we found that even the remote rural patients from Mizoram have read and come for treatment especially after reading the following
http://mdcurrent.in/patients/prostate-surgeries-in-rural-areas/
http://mdcurrent.in/patients/small-urinary-tract-stones-the-available-options-in-rural-areas/
http://mdcurrent.in/patients/what-is-new-about-appendix-surgeries/
May God bless your efforts
J. Gnanaraj
CHW Data for Decision Making – Challenges for scale-up of CHW programs – Fragmentation, comprehensiveness, data, funding, disability, intersectoral collaboration
Many thanks for stimulating this open discussion on CHWs – a critical cadre in resolving the health workforce crisis in Africa… and beyond.
In IAPB (the International Agency for the Prevention of Blindness) we have been making use of various cadres of CHWs for many years, most notably, Community Directed Distributors (CDDs) of Zithromax for trachoma control and Ivermectin for oncho/river blindness.
Last year, as part of our comprehensive response to the workforce crisis (ophthalmologists, optometrists, allied eye health professionals, Primary Eye Care Workers and CHWs), we undertook a situation analysis, in 23 countries in Africa, of the role of CHWs in eye health.
The results were quite staggering as we discovered 59 different cadres playing a role, in one way or another, in promoting eye health at the community level.
The report, which has just been finalised, is attached [*] along with 2 of the most relevant appendices – on classifications and a Ghana case study. The Report, along with all the appendices will be available in the next 2 weeks on the IAPB Africa website.
Alongside this work, one of our cadre-specific Working Groups has also completed a provisional set of core competencies for the eye health component of the CHW workforce, which we are currently validating with expert groups in WHO-Afro.
In a sense, all this is by way of background to our response to the discussion of the week – What are the most pressing challenges in the scale-up of CHW programmes today ?
Our Response = 6 Key issues:
1. Fragmentation: Even within a hitherto vertical programme such as eye health we are constantly striving, as IAPB, to coordinate the activities of our many member agencies and to align a collective response with existing CHW initiatives.
2. Comprehensiveness: According to 3 recent studies in Kenya, Cameroon and Nigeria, ocular morbidities (particularly conjunctivitis and presbyopia) account for 15-20% of all health problems faced by communities in addition to blindness at 1%, low vision at 1% and uncorrected refractive error at 4%. In other words, eye health is a major challenge at the community level and we all need to work to ensure that any new curriculum for CHWs includes the component of eye health.
3. Data: While we have excellent figures for the number of CDDs due to the long-running oncho and trachoma control programmes, much less is known about the numbers, distribution, retention, training, and impact of CHWs who have been trained to deliver eye health services, as our report makes clear. Our response has been to develop a database (the IADb) of over 300 eye health indictors, aligned with DHIS2 and the African Health Observatories, to capture basic data at the community and primary levels.
4. Funding: Various approaches to scaling-up the CHW workforce are being implemented but the capacity to take them to scale remains elusive. IAPB, with 40 active members in Africa, can play a part in scaling-up but cannot take on the job on its own. We need to see a greater government commitment to a comprehensive process, which must include all causes of mortality and morbidity.
5. Disability: In eye health we would also be looking at the role of the community worker in disability eg finding the blind child, inclusive education of the irreversibly blind child and rehabilitation of the blind adult.
6. Inter-sectoral collaboration: This is critical at community level with respect, in particular, to water and sanitation in trachoma control.
I do hope this contribution to the discussion is useful and we look forward to comments, constructive criticism and guidance as we move forward together.
As always
Ronnie Graham
Director, HReH,
IAPB Africa
HIFA profile: Ronnie Graham is Director, Human Resources for Eye Health, IAPB Africa, and is based in Durban, South Africa. Professional interests: Human resources for eye health in Africa, advocacy, HMIS, research, primary health care, mHealth, Francophone and Lusophone Africa, faculty and training programmes, the GHWA-HWAI (Global Health Workforce Alliance – Health Workers Advocacy Initiative) and health economics. rgraham AT iapb.org
[*Note from HIFA moderator: HIFA does not carry attachments. Please contact Ronnie direct. Thanks, Neil PW]
Master of Medical Informatics …still open for applicants. Please apply!
Where: Pfarrkirchen, Germany
Costs: no tuition fees
Apply: https://www.th-deg.de/en/agw/courses/mi-m-en
Objectives:
The Master’s programme Medical Informatics provides bachelor or diploma graduates a theoretical basis to reinforce the knowledge they have gained thus far in order to meet the requirements of modern-day research and development tasks. The programme is offered through the faculty of Applied Health Sciences.
The Master of Medical Informatics builds on knowledge gained in bachelor or diploma programmes. Graduates will be qualified to perform evidence-based work in research and development departments in the areas of telematics, telemedicine, and eHealth, as well as in the area of service provision within the health industry at the national and international level. In addition, particularly qualified students should gain the theoretical basis needed for a promotion or for work in academic fields.
—
Anna E. Schmaus-Klughammer (LLB hons) President
HIFA profile: Anna E. Schmaus-Klughammer is president of the association “One World Medical Network”.
The goal of the association is to improve medical care in LMICs (Low and Middle Income Countries).
Our activities start from building primary and specialized health care facilities and continue to organize national cancer screening with connections to national and international expert doctors using telemedicine networks. Training of medical personnel is also an important part of the work of the association.
One World Medical Network e.V.
Ulrichsbergerstra? 17
94469 Deggendorf
Deutschland/Germany
Fon +49 991 – 99133913
Fax +49 991 – 991339 50
New free online course: The Informed Health Consumer
Cardiff University is running a new MOOC (Massive Open Online Course) on the FutureLearn platform from Monday 7 September. It’s called The Informed Health Consumer: Making Sense of Evidence. [*see note below]
This free course is aimed at a lay audience and will be useful for people who want to find out more about a medical condition or those considering studying a health-related subject at university. It will also interest those who want to improve their knowledge of a health-related issue.
Over four weeks, the course will:
· Look at the factors that affect the reliability of evidence;
· Provide practical help on how to find the best evidence;
· Improve understanding of the terminology of health research;
· Provide some simple tools to help judge whether it’s reliable.
Thanks
Fiona Morgan
Lecturer – School of Healthcare Sciences / Darlithydd – Ysgol Gwyddorau Gofal Iechyd
Systematic Reviewer, SURE – University Library Service / Adolygydd Systematig, SURE – Gwasanaeth Llyfrgell y Brifysgol
Cardiff University / Prifysgol Caerdydd
Check out the latest Cardiff University MOOC from 7th September: The Informed Health Consumer: Making Sense of Science https://www.futurelearn.com/courses/informed-health-consumer
Estimating the lost benefits of not implementing a visual inspection with acetic acid screen and treat strategy for cervical cancer prevention in South Africa
Abstract
INTRODUCTION
South Africa has had a national cervical cancer screening policy (2002) based on the Pap (Papanicolaou) smear for more than 10 years which has not been effective. Cancer of the cervix remains a very common cancer among women in South Africa.
Zambia was able to integrate Visual Inspection with Acetic acid screening for cervical cancer and treatment successfully within its public sector HIV/AIDS treatment program while minimizing the need for additional resources.
The aim of this study was to quantify the impact on cervical cancer high grade pre-cursor lesions, new cases and deaths from cervical cancer had South Africa implemented a nurse driven Visual Inspection with Acetic based screen and treat strategy like Zambia (Botswana and Zimbabwe) did.
METHODS
Using publicly available published evidence based data a statistical model was developed to estimate the aforementioned outcomes that could have been prevented in South Africa had the country followed Zambia’s strategy.
RESULTS
South Africa could have prevented over five years at least 3 300 high-grade cervical pre-cursor lesions, and assuming one round of Visual Inspection with Acetic screening and treatment, 50 cases of cervical cancer and 40 deaths from cervical cancer.
CONCLUSION
Had South Africa adopted a pragmatic low cost method to prevent cervical cancer like Zambia (Botswana and Zimbabwe) did, substantial morbidity and mortality from cervical cancer would have been prevented. Important public health lessons for politicians, policy makers and others can be drawn from this missed opportunity.
South Africa has had a national cervical cancer screening policy (2002) based on the Pap (Papanicolaou) smear for more than 10 years which has not been effective. Cancer of the cervix remains a very common cancer among women in South Africa.
Zambia was able to integrate Visual Inspection with Acetic acid screening for cervical cancer and treatment successfully within its public sector HIV/AIDS treatment program while minimizing the need for additional resources.
The aim of this study was to quantify the impact on cervical cancer high grade pre-cursor lesions, new cases and deaths from cervical cancer had South Africa implemented a nurse driven Visual Inspection with Acetic based screen and treat strategy like Zambia (Botswana and Zimbabwe) did.
METHODS
Using publicly available published evidence based data a statistical model was developed to estimate the aforementioned outcomes that could have been prevented in South Africa had the country followed Zambia’s strategy.
RESULTS
South Africa could have prevented over five years at least 3 300 high-grade cervical pre-cursor lesions, and assuming one round of Visual Inspection with Acetic screening and treatment, 50 cases of cervical cancer and 40 deaths from cervical cancer.
CONCLUSION
Had South Africa adopted a pragmatic low cost method to prevent cervical cancer like Zambia (Botswana and Zimbabwe) did, substantial morbidity and mortality from cervical cancer would have been prevented. Important public health lessons for politicians, policy makers and others can be drawn from this missed opportunity.
Friends at Work? Not So Much
 ONCE, work was a major source of friendships. We took our families to company picnics and invited our colleagues over for dinner. Now, work is a more transactional place. We go to the office to be efficient, not to form bonds. We have plenty of productive conversations but fewer meaningful relationships. In 1985, about half of Americanssaid they had a close friend at work; by 2004, this was true for only 30 percent. And in nationally representative surveys of American high school seniors, the proportion who said it was very important to find a job where they could make friends dropped from 54 percent in 1976, to 48 percent in 1991, to 41 percent in 2006…..more
ONCE, work was a major source of friendships. We took our families to company picnics and invited our colleagues over for dinner. Now, work is a more transactional place. We go to the office to be efficient, not to form bonds. We have plenty of productive conversations but fewer meaningful relationships. In 1985, about half of Americanssaid they had a close friend at work; by 2004, this was true for only 30 percent. And in nationally representative surveys of American high school seniors, the proportion who said it was very important to find a job where they could make friends dropped from 54 percent in 1976, to 48 percent in 1991, to 41 percent in 2006…..more
WHO Bulletin: Maximizing the impact of community-based practitioners in the quest for universal health coverage
CITATION: Maximizing the impact of community-based practitioners in the quest for universal health coverage
James Campbell, Kesetebirhan Admasu, Agnes Soucat & Sheila Tlou.
Correspondence to James Campbell (email: campbellj@who.int).
Bulletin of the World Health Organization 2015;93:590-590A. doi: http://dx.doi.org/10.2471/BLT.15.162198
EXTRACTS (selected by Neil PW)
‘McPake et al. report that investment in these types of health workers can be a cost-effective approach, in certain contexts and under certain circumstances…’
‘The terms “frontline health workers” and “community health workers” are often used in a non-specific way and can confuse the evidence base. The term “frontline” is not a classification recognized by the World Health Organization (WHO) or the International Labour Organization (ILO). Even the official classification of community health workers can refer to a diverse typology of lay and educated, formal and informal, regulated and unregulated, paid and unpaid health workers. Different policies relating to individual cadres, their scope of practice, education and relation to the health system undermine efforts to strengthen service delivery at community level…’
‘WHO’s Global strategy on human resources for health: workforce 2030… recognizes the potential of involving community-based, mid-level and advanced practitioners as part of a multi-disciplinary health workforce that offers people-centred, integrated primary health services.’
‘Guidelines on the role, education and integration of community-based practitioners are being prepared by WHO for publication in 2017. These guidelines will provide governments and development partners with evidence-based recommendations on community-based practitioners, including potential returns on investment. These guidelines are intended to support universal health coverage and the achievement of the Sustainable Development Goals.’
—
Best wishes, Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
WHO Bulletin: Cost–effectiveness of community-based practitioner programmes in Ethiopia, Indonesia and Kenya
Please find below the citation and abstract of a paper in the September 2015 issue of the WHO Bulletin. Full text is freely available here: http://www.who.int/bulletin/volumes/93/9/14-144899/en/
CITATION: Cost-effectivenesss of community-based practitioner programmes in Ethiopia, Indonesia and Kenya
Barbara McPake, Ijeoma Edoka, Sophie Witter, Karina Kielmann, Miriam Taegtmeyer, Marjolein Dieleman, Kelsey Vaughan, Elvis Gama, Maryse Kok, Daniel Datiko, Lillian Otiso, Rukhsana Ahmed, Neil Squires, Chutima Suraratdecha & Giorgio Cometto
doi: 10.2471/BLT.14.144899
Cost–effectiveness of community-based practitioner programmes in Ethiopia, Indonesia and Kenya
Barbara McPake, Ijeoma Edoka, Sophie Witter, Karina Kielmann, Miriam Taegtmeyer, Marjolein Dieleman, Kelsey Vaughan, Elvis Gama, Maryse Kok, Daniel Datiko, Lillian Otiso, Rukhsana Ahmed, Neil Squires, Chutima Suraratdecha & Giorgio Cometto
Objective: To assess the cost–effectiveness of community-based practitioner programmes in Ethiopia, Indonesia and Kenya.
Methods: Incremental cost–effectiveness ratios for the three programmes were estimated from a government perspective. Cost data were collected for 2012. Life years gained were estimated based on coverage of reproductive, maternal, neonatal and child health services. For Ethiopia and Kenya, estimates of coverage before and after the implementation of the programme were obtained from empirical studies. For Indonesia, coverage of health service interventions was estimated from routine data. We used the Lives Saved Tool to estimate the number of lives saved from changes in reproductive, maternal, neonatal and child health-service coverage. Gross domestic product per capita was used as the reference willingness-to-pay threshold value.
Findings: The estimated incremental cost per life year gained was 82 international dollars ($)in Kenya, $999 in Ethiopia and $3396 in Indonesia. The results were most sensitive to uncertainty in the estimates of life-years gained. Based on the results of probabilistic sensitivity analysis, there was greater than 80% certainty that each programme was cost-effective.
Conclusion: Community-based approaches are likely to be cost-effective for delivery of some essential health interventions where community-based practitioners operate within an integrated team supported by the health system. Community-based practitioners may be most appropriate in rural poor communities that have limited access to more qualified health professionals. Further research is required to understand which programmatic design features are critical to effectiveness.
—
Best wishes, Neil
Let’s build a future where people are no longer dying for lack of healthcare knowledge – Join HIFA: www.hifa2015.org
